Introduction
When you hear "hospital switchboard," two systems come to mind: the communications console where operators route phone calls, and the electrical power distribution switchboard that keeps every clinical system, life-safety device, and critical load energized 24/7. This article focuses squarely on the latter—the electrical infrastructure layer that hospital administrators, facility engineers, and electrical contractors depend on to maintain uninterrupted power where equipment failure directly affects patient outcomes.
Hospitals are unforgiving for electrical power distribution. A momentary interruption can compromise ventilators, surgical lighting, patient monitoring systems, and infusion pumps. Unlike office buildings or data centers, healthcare facilities run around the clock with no tolerance for outages—planned or unplanned. The hospital electrical switchboard is a mission-critical asset, full stop.
This article covers what hospital electrical switchboards are, why healthcare power distribution differs from every other building type, the unique compliance demands of NFPA 99 and NEC Article 517, modern infrastructure challenges, and what engineers and facility teams should prioritize when specifying one.
TLDR:
- Hospital switchboards distribute power to clinical departments with strict separation between life-safety and normal circuits
- NFPA 99 and NEC Article 517 require essential electrical systems (EES) with 10-second maximum transfer times to backup power
- Hospitals use 3x more energy per square foot than typical office buildings, with loads growing due to imaging equipment, robotics, and on-site data centers
- UL 891-certified switchboards require draw-out breakers, integrated metering, arc flash protection, and BABA compliance for federal projects
- Custom-configured hospital switchboards require 4–6 week lead times — shorter with manufacturers that build in-house
What Is a Hospital Electrical Switchboard?
A hospital electrical switchboard is a low-voltage power distribution assembly that receives power from the utility or on-site generation and distributes it to branch circuits and sub-panels throughout the facility. It's governed by UL 891, the U.S. product standard for dead-front distribution switchboards rated 600V or less, covering construction and test requirements for wiring, clearances, insulation, and protective device operation.
Core components include:
- Main busbars (copper or aluminum conductors carrying the primary electrical load)
- Circuit breakers or fuses (providing overcurrent and fault protection)
- Metering equipment (tracking real-time demand, power factor, and energy consumption)
- Protective relays (detecting and isolating ground faults, short circuits, and arc flash events)
- Feeder disconnect means (enabling safe isolation of downstream circuits for maintenance)
These components work together to route and control electrical loads across the building — from operating rooms and ICUs to imaging suites and pharmacy cleanrooms. These components work together to route and control electrical loads across the building — from operating rooms and ICUs to imaging suites and pharmacy cleanrooms. Understanding how they're arranged within the broader power system clarifies why switchboard selection matters at every tier.
Where the Switchboard Fits in the Power Hierarchy
In a typical hospital electrical system, the switchboard sits between the utility transformer (or generator output) and downstream distribution panels serving individual departments. The hierarchy flows as follows:
- Utility transformer or generator feeds power to the main switchboard
- Main switchboard distributes power to sub-distribution panels
- Sub-distribution panels serve branch circuits in specific departments (OR, ICU, imaging, pharmacy)
- Branch circuits power individual equipment and receptacles

Switchboard vs. Switchgear: Understanding the Difference
| Feature | UL 891 Switchboard | UL 1558 Switchgear |
|---|---|---|
| Breaker type | UL 489 molded case (MCCB) or fixed-frame | UL 1066 low-voltage power circuit breakers (draw-out) |
| Busbars | Non-insulated | Insulated |
| Construction | Group-mounted, less compartmentalization | Individually fixed, metal-enclosed, compartmentalized |
| Withstand rating | 3-cycle withstand | High short-time withstand |
| Typical capacity | Up to 6,000A | Up to 6,000A+ (draw-out configuration) |
| Maintenance | May require full busbar shutdown | Draw-out allows maintenance without full shutdown |
| Cost | Mid-range | Highest |
Hospitals commonly use UL 891 switchboards for main and sub-distribution applications at 600V and below, which covers the vast majority of healthcare facility power systems.
Modern Hospital Switchboards as Monitoring and Control Points
Today's hospital switchboards integrate far more than basic circuit protection. Modern assemblies serve as active monitoring and control points across the facility. Key capabilities include:
- Integrated metering — tracks demand, power factor, harmonic distortion, and consumption by department for energy management and departmental billing
- Predictive maintenance data — consumption trends flag anomalies before they cause unplanned outages
- Ground fault protection — detects and isolates fault conditions before they escalate into equipment damage
- Arc flash detection — gives facility teams immediate visibility into high-energy fault events that pose direct safety risks
Why Hospital Power Distribution Is Unlike Any Other Facility
Essential Electrical Systems (EES) and Code-Mandated Separation
NFPA 99 (Health Care Facilities Code) and NEC Article 517 define the concept of essential electrical systems (EES): hospitals must maintain separate, independently supplied circuits for life safety, critical, and equipment branches. This shapes every decision in switchboard design and configuration.
The three branches of the EES for Type 1 facilities:
| Branch | Priority | Key Loads | Transfer Time |
|---|---|---|---|
| Life Safety | Highest | Exit signs, egress lighting, fire alarms, hospital communications, elevator cab lighting/control | 10 seconds maximum |
| Critical | High | Task lighting and receptacles in patient care areas (ICU, OR, ER, PACU), nurse call systems, blood/tissue banks, isolated power systems | 10 seconds maximum |
| Equipment | Sequenced | Central suction, compressed air, sump pumps, smoke control, kitchen hood systems, select elevators, HVAC for critical areas | May be delayed or sequenced |
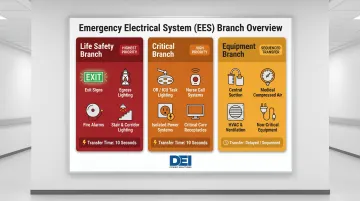
For emergency loads over 150 kVA, the NEC requires the system be divided into three branches with separate automatic transfer switches.
The Consequences of Power Failure in Healthcare
Even a momentary interruption can compromise patient safety. A 2025 study published in JAMA Network Open analyzing the CrowdStrike IT outage found that 21.8% of technology service disruptions (239 out of 1,095 services) had direct patient safety implications across affected hospitals.
NFPA 99, Section 6.4.3.1 mandates that Life Safety and Critical branches be automatically restored to operation within 10 seconds of interruption of the normal source. That 10-second ceiling drives every aspect of hospital switchboard configuration and coordination with automatic transfer switches.
24/7/365 Operation with No Tolerance for Downtime
Meeting that standard also means designing for continuous operation. Hospitals run around the clock, maintenance windows are extremely narrow, and unplanned outages are not an option. Switchboards must support:
- Hot-swap component replacement
- Draw-out breaker configurations (enabling maintenance without full busbar shutdown)
- Full redundancy on critical feeders
High and Diverse Electrical Load Profile
Modern hospitals present uniquely demanding electrical challenges:
- MRI machines and CT scanners draw large inrush currents
- Surgical suites require isolated ground circuits to protect patients from microshock hazards
- Data centers and EHR server rooms need stable, clean power
- Cooling systems account for nearly 25% of total hospital electricity consumption
According to the Department of Energy, hospitals use more than 3x the energy per square foot compared to typical office buildings. EIA 2018 CBECS data shows inpatient healthcare buildings have an energy use intensity (EUI) of 193.3 thousand BTU per square foot—more than double outpatient facilities (82.0). Inpatient facilities account for 68% of healthcare sector electricity consumption despite representing only 6% of healthcare buildings.
That density of load is compounded by a growing push toward on-site generation. Hospitals increasingly integrate rooftop solar, battery energy storage, and combined heat-and-power (CHP) systems to improve resilience and meet sustainability goals. 229 U.S. hospitals currently use CHP systems, totaling 745 MW of installed electric capacity—roughly 3.3 MW per hospital on average. An estimated 7.3 GW of additional CHP technical potential exists across more than 6,000 U.S. hospitals.

Each of these additions introduces new complexity to the switchboard's role: bidirectional power flows, anti-islanding requirements, paralleling capability, and coordination with utility interconnection requirements all become part of the design equation.
Key Functions of a Hospital Switchboard
Power Distribution and Load Segregation
The switchboard physically separates normal power from essential electrical system branches (life safety, critical, and equipment), ensuring that a fault on one branch cannot cascade to life-critical circuits. This segregation is not optional—it's a core requirement of NFPA 99 and NEC Article 517.
Overcurrent Protection and Fault Isolation
Circuit breakers and protective relays within the switchboard detect and isolate overcurrents, short circuits, and ground faults before they can damage downstream equipment or create safety hazards for patients and staff.
NEC 517.17 requires a second level of ground fault protection on all feeders whenever the service requires ground fault protection, preventing a single ground fault from disabling the entire system.
Transfer Switching Coordination
The switchboard coordinates with automatic transfer switches (ATS) that shift essential loads to generator power during a utility outage. Proper sequencing logic in the switchboard is critical to staying within the 10-second transfer time mandate.
Sequencing follows a defined priority order:
- Life Safety branch transfers first — emergency lighting, alarms, egress systems
- Critical branch follows — operating rooms, ICUs, nurse call systems
- Equipment branch loads come last, staged to stay within generator startup capacity
Metering, Monitoring, and Power Quality
Integrated metering modules within modern hospital switchboards track:
- Real-time demand and peak load
- Power factor and reactive power
- Harmonic distortion (particularly important given the prevalence of nonlinear medical equipment loads)
- Energy consumption by department
Facility managers use this data to catch equipment anomalies early, allocate costs by department, and avoid demand-charge spikes during peak operating hours.
Grounding and Patient Safety
Healthcare settings have special grounding requirements to protect patients from microshock hazards (leakage currents as low as 10 microamperes can cause ventricular fibrillation in patients with direct cardiac conduction pathways).
Key grounding systems in hospitals:
- Isolated power systems use ungrounded configurations in wet procedure locations, keeping power flowing even when a single fault occurs
- Line Isolation Monitors (LIMs) continuously measure the impedance of each line to ground, flagging degraded insulation before it becomes a hazard
- Low-impedance equipment grounding bonds all conductive surfaces in patient care areas to a common reference, minimizing voltage differentials that could cause microshock
NEC 517.160 governs isolated power systems. When the total hazard current exceeds a threshold (typically 5 mA), the LIM triggers a visible and audible alarm without interrupting power, allowing clinical staff to continue a procedure safely while being alerted to degraded insulation.
Compliance and Safety Standards Every Hospital Switchboard Must Meet
Hospital switchboards must satisfy several overlapping codes and standards — each targeting a different layer of safety, from system design to daily maintenance. Here's what contractors, engineers, and facility teams need to know.
NFPA 99 (Health Care Facilities Code)
Current edition: NFPA 99, 2024 Edition. This code sets risk-based requirements for healthcare electrical systems, with direct implications for how hospital switchboards are designed, maintained, and tested. The electrical systems chapter covers:
- Performance and testing requirements for normal and essential electrical systems
- Risk category classifications that determine equipment redundancy levels
- Maintenance intervals and documentation standards for critical power infrastructure
NEC Article 517 (Health Care Facilities)
Current edition: NEC 2023 (NFPA 70), with an effective date of September 1, 2022. Article 517 applies to "buildings, portions of buildings, or mobile enclosures in which human medical, dental, psychiatric, nursing, obstetrical or surgical care is provided." It defines the three power branches within the EES and their specific wiring and connection requirements.
UL 891 Listing Requirement
UL 891 listing confirms a switchboard meets safety and construction requirements for dead-front switchboards rated 600V and below. Hospital purchasing teams and Authorities Having Jurisdiction (AHJs) routinely require UL 891-listed switchboards as evidence of third-party testing and code compliance.
Under UL's General Coverage Program, approved manufacturers can apply the UL Mark at their factories — meaning the listing reflects ongoing factory-level quality controls, not just a one-time sample submission. For procurement teams, that's a meaningful distinction when specifying equipment for critical care environments.
NFPA 70E Arc Flash Hazard Analysis
Beyond installation, ongoing maintenance introduces arc flash exposure risk. NFPA 70E, 2024 Edition (Standard for Electrical Safety in the Workplace), Article 130.5 requires an arc flash risk assessment for any work within the arc flash boundary.
Required PPE scales with incident energy levels:
| PPE Category | Minimum Arc Rating | Incident Energy Range |
|---|---|---|
| Category 1 | 4 cal/cm² | >1.2 up to 4 cal/cm² |
| Category 2 | 8 cal/cm² | >4 up to 8 cal/cm² |
| Category 3 | 25 cal/cm² | >8 up to 25 cal/cm² |
| Category 4 | 40 cal/cm² | >25 up to 40 cal/cm² |
Above 40 cal/cm², energized work is generally prohibited due to lethal blast pressure risk regardless of thermal PPE.
Switchboard design has a direct impact on these risk levels. Features that reduce incident energy — and therefore PPE requirements — include:
- Current-limiting fuses and breakers
- Zone-Selective Interlocking (ZSI), which allows local breakers to trip instantaneously for faults in their zone
- Differential protection for fast fault clearing
- Breaker coordination studies to verify selective tripping under fault conditions
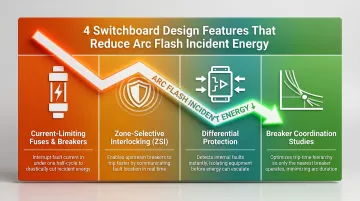
Specifying these features upfront reduces long-term exposure risk for maintenance personnel and can lower facility insurance costs.
Modern Challenges in Hospital Power Infrastructure
Aging Infrastructure and Capacity Constraints
According to the American Hospital Association, nearly one-third of rural hospitals reported an average age of plant of 15 years or older. Total hospital beds in the U.S. have declined by 33% since 1980, while regulatory requirements have expanded.
Financial pressures have caused many hospitals to "pause capital spending, thereby delaying necessary maintenance even further."
Hospital electrical loads have climbed steadily over the past decade as facilities add imaging suites, robotic surgery systems, on-site data centers, and EV charging stations. Many facilities are operating switchboards that predate current code requirements and may lack adequate capacity, arc flash protection, or modern monitoring capabilities.
Construction Lead Time Pressures
The 2025 ASHE/HFM Hospital Construction Survey found that 18% of surveyed hospitals have electrical switchgear or transformers currently under construction, with electric switchgear facing "exceedingly long lead times." Some facilities are ordering switchgear before finalizing design drawings to mitigate schedule risk.
Traditional custom switchgear lead times stretch from 52 to 100+ weeks for complex configurations, which can hold up certificate of occupancy and department openings—directly impacting patient care capacity and hospital revenue.
Integrating Backup and Renewable Energy Sources
Long lead times compound an already difficult problem: hospitals that are also adding battery storage or solar generation face additional re-engineering demands on top of schedule pressure. Existing switchboard configurations may need to be redesigned to handle new sources, anti-islanding requirements, and bidirectional metering.
Kaiser Permanente Ontario Medical Center, for example, installed a microgrid with 2 MW of on-site solar generation and 9 MWh of non-lithium battery storage capacity—a configuration where the switchboard, transfer switches, paralleling gear, and utility interconnection protection all had to be specified and sequenced together from the start of design.
What to Look for When Specifying a Hospital Switchboard
Custom Configuration and Engineering Support
Hospital switchboards are rarely off-the-shelf. They must be engineered to the facility's specific voltage class, bus ampacity, feeder count, load schedule, and physical footprint. Key specification considerations include:
- Voltage class matched to facility design: 120/240V, 208Y/120V, 480V, 480Y/277V, or 415/240V
- Bus ampacity sized from 400A to 4,000A, with growth margins built in for future loads
- Draw-out breaker configurations that allow maintenance without shutting down the entire busbar
- Harmonic distortion tolerance, since nonlinear medical equipment loads create harmonics that must be managed
- SCADA/BMS integration for real-time monitoring, energy management, and predictive maintenance
Engineering support from the manufacturer matters as much as the hardware itself. Prioritize companies that provide configuration guidance, load schedule review, and complete documentation packages for AHJ review.
Short Lead Times and Domestic Manufacturing
Healthcare construction projects operate on tight schedules, and switchboard delays can hold up certificate of occupancy and department openings. Look for manufacturers with:
- In-house fabrication capability
- Proven fast-turn fulfillment (4–6 week lead times vs. industry-standard 52–100 weeks)
- Vertically integrated manufacturing to minimize supply chain dependencies
DEI Power manufactures UL 891-certified switchboards at a 50,000 sq. ft. facility in Ontario, California, with typical lead times of 4–6 weeks and nationwide delivery in 3–5 business days — a meaningful gap compared to the 52–100 week industry standard.

BABA Compliance for Federally Funded Projects
The Build America, Buy America Act (Pub. L. No. 117-58), enacted November 15, 2021, applies to federally funded hospital construction (including HHS, HRSA, and USDA programs). Three core requirements:
- All iron and steel must be produced in the U.S. (all manufacturing processes through coatings)
- Manufactured products (including switchboards) must be manufactured in the U.S. with >55% U.S.-origin component cost
- All construction materials must be manufactured in the U.S.
DEI Power manufactures and assembles switchgear in the United States with BABA-compliant construction, providing compliance certifications and project-specific documentation to simplify federal procurement.
Full Documentation for Commissioning and AHJ Review
Proper documentation accelerates commissioning and AHJ approval. Look for manufacturers that supply:
- Complete submittal packages with one-line diagrams, panel schedules, and equipment specifications
- UL 891 certification documentation
- Arc flash hazard analysis and labeling per NFPA 70E
- Seismic certification (UBC, CBC, IBC compliance)
- Factory acceptance test (FAT) reports
Frequently Asked Questions
What is a hospital switchboard?
A hospital switchboard refers to one of two distinct systems: an electrical power distribution switchboard (governed by UL 891) that routes electricity from utility or generator sources to clinical departments, or a communications switchboard that handles phone routing and paging. The two systems are entirely separate.
What does a hospital switchboard do?
A hospital electrical switchboard receives power from the utility or generator, distributes it to branch circuits serving clinical departments, and provides overcurrent and fault protection. It separates life-safety circuits from normal power per NFPA 99 and NEC Article 517, enabling safe maintenance and fast fault isolation.
What does 2222 mean in a hospital?
2222 is the standardized internal telephone number for cardiac arrest (crash) calls in NHS hospitals, promoted by the European Resuscitation Council for pan-European adoption. Dialing 2222 from any internal phone summons the resuscitation team — a communications switchboard function entirely separate from electrical power distribution.
What electrical codes and standards apply to hospital switchboards?
NFPA 99 (Health Care Facilities Code) defines essential electrical system requirements; NEC Article 517 specifies wiring methods for healthcare occupancies; UL 891 governs the construction and testing of low-voltage switchboards; and NFPA 70E addresses arc flash safety for maintenance personnel. All four standards are mandatory for hospital electrical systems.
What is the difference between a switchboard and switchgear in a hospital?
Switchboards (UL 891) are open, front-accessible assemblies used at 600V and below for main and sub-distribution, while switchgear (UL 1558 or ANSI C37) is metal-enclosed draw-out equipment for medium-voltage, utility-side distribution. Hospitals typically use both, depending on the point in the power system.
How does a hospital maintain power during an outage?
Hospitals use automatic transfer switches (ATS) coordinated with the switchboard to shift essential electrical loads to on-site emergency generators within 10 seconds (as required by NFPA 99). Some facilities also add uninterruptible power supplies (UPS) for zero-transfer-time protection on the most sensitive equipment such as surgical robotics and data center infrastructure.